7312 - Cirrhosis of the liver
DBQ: Link to Index of DBQ/Exams by Disability for DC 7312
Acronym: PBC
Definition
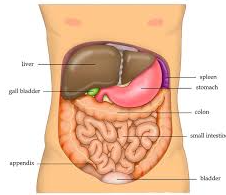
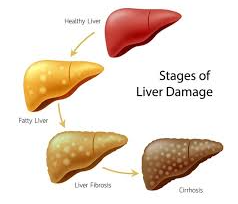
The liver is a large organ situated in the upper abdomen on the right side. Cirrhosis of the liver is a long-standing, degenerative disease characterized by deterioration and destruction of essential parts of the organ; invasion of the structure and blood vessels fibrous tissue, and infiltration of the cells by fat.
{kind=link}
{kind=link}
Etiology
The condition is more common in men than women. Cirrhosis may be caused by various factors including nutritional deficiencies due to a lack of protein, choline or methionine; infection caused by a virus or bacterium; toxins or poisons, including alcohol, carbon tetrachloride and phosphorus; altered immune response; biliary obstruction; and vascular disturbance. The cause may vary with the type of cirrhosis. The causes may include malnutrition and chronic excessive alcohol ingestion, referred to as Laennec's cirrhosis. Cirrhosis may result from bile duct disease that is referred to as biliary cirrhosis. Various types of hepatitis may cause the disease (postnecrotic cirrhosis), or it may be caused by metabolic disorders such as galactosemia, or hemochromatosis (pigment cirrhosis).
Signs & Symptoms
{kind=link}
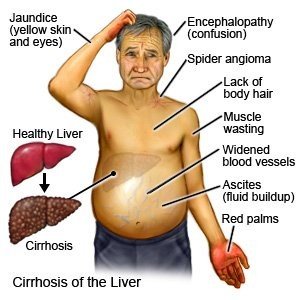
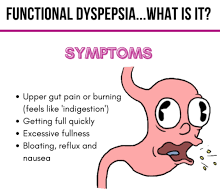
Cirrhosis of the liver affects many body systems. The symptoms may include loss of appetite; chronic dyspepsia; indigestion; nausea; vomiting; constipation or diarrhea; palpable liver or spleen; elevated temperature; and abdominal pain. Pleural effusion and limited thoracic expansion can develop. Easy bruising, frequent nosebleeds, bleeding gums, hemorrhage from esophageal varices, and anemia are also present. In addition, manifestations may include: extreme dryness of the skin; pruritus; poor skin turgor; abnormal pigmentation; telangiectasis; spider angiomas; palmar erythema; distended abdominal vessels; umbilical hernia; hepatomegaly; thigh and leg edema; ascites, and, possibly, jaundice. Other symptoms may include menstrual irregularities, testicular atrophy, gynecomastia, and loss of chest and axillary hair.
{kind=link}
{kind=link}
With progressive hepatic encephalopathy, the developments include: lethargy; behavioral or personality changes; slurred speech; involuntary jerking movements (asterixis), referred to as liver flap or liver tremors; peripheral neuritis; paranoia; hallucinations; mental dullness; and coma.
{kind=link}
Tests
Liver biopsy and liver scans are among the diagnostic measures implemented. Additional tests used to confirm the diagnosis include cholecystography; cholangiography; spleno portal venography; percutaneous transhepatic cholangiography; blood tests; glucose tolerance tests; galactose tolerance and urine bilirubin tests; and fecal or urine urobilinogen level checks or both.
{kind=link}
{kind=link}
Treatment
Supportive treatment may include: (1) removing or alleviating the underlying causes, such as the toxic agents, (2) prevention of further damage to the liver, and (3) prevention and/or treatment of associated complications. Major emphasis is placed on nutrition. As a last resort, if other treatment plans are unsuccessful, a liver transplant may be required.
Residuals
It is difficult to estimate residuals because of the many causes of the condition. Residuals will vary from no residuals to any combination of the signs and symptoms and associated major complications (portal hypertension with variceal bleeding, liver failure, coma, and death).
Special Considerations
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
-
If the Veteran is a former prisoner of war and was interned or detained for not less that 30 days, this disease shall be service connected if manifest to a degree of disability of 10 percent or more at any time after discharge or release from active military, naval, or air service even though there is no record of such disease during service, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [Disease subject to presumptive service connection], 38 CFR 3.309 (c)].
-
Service connection shall be granted although not otherwise established as incurred in or aggravated by service if manifested to a compensable degree within the applicable time limits under 38 CFR 3.307 following service in a period of war or following peacetime service on or after January 1, 1947, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied. [38 CFR 3.309(a)]
Notes
-
Rate hepatocellular carcinoma occurring with cirrhosis under DC 7343 (Malignant neoplasms of the digestive system, exclusive of skin growths) in lieu of DC 7312.
-
Biochemical studies, imaging studies, or biopsy must confirm liver dysfunction (including hyponatremia, thrombocytopenia, and/or coagulopathy).
-
Rate condition based on symptomatology where the evidence does not contain a Model for End-Stage Liver Disease score.
-
Ratings under diagnostic codes 7301 to 7329, inclusive, 7331, 7342, and 7345 to 7348 inclusive will not be combined with each other. A single evaluation will be assigned under the diagnostic code which reflects the predominant disability picture, with elevation to the next higher evaluation where the severity of the overall disability warrants such elevation. [38 CR 4.114]
-
There are diseases of the digestive system, particularly within the abdomen, which, while differing in the site of pathology, produce a common disability picture characterized in the main by varying degrees of abdominal distress or pain, anemia and disturbances in nutrition. Consequently, certain coexisting diseases in this area, as indicated in the instruction under the title “Diseases of the Digestive System,” do not lend themselves to distinct and separate disability evaluations without violating the fundamental principle relating to pyramiding as outlined in 38 CFR 4.14. [38 CFR 4.113]
-
For purposes of evaluating conditions in 38 CFR 4.114, the term “substantial weight loss” means a loss of greater than 20 percent of the individual's baseline weight, sustained for three months or longer; and the term “minor weight loss” means a weight loss of 10 to 20 percent of the individual's baseline weight, sustained for three months or longer. The term “inability to gain weight” means that there has been substantial weight loss with inability to regain it despite appropriate therapy. “Baseline weight” means the average weight for the two-year-period preceding onset of the disease. [38 CFR 4.112]